White Blotches in Back of Throat: Causes, Symptoms, and Evidence-Based Treatments

Noticing an unusual change in your mouth or throat can be unsettling, especially when you spot unexpected discoloration during a routine mirror check. Discovering white blotches in back of throat often triggers immediate concern, but understanding the underlying causes can help you navigate next steps with clarity and confidence. This comprehensive guide explores the clinical, environmental, and lifestyle factors that contribute to these visible lesions, providing evidence-based insights aligned with current medical guidelines. Whether you are experiencing mild discomfort or more pronounced symptoms, knowing when to manage the condition at home versus when to consult an ear, nose, and throat specialist is essential for optimal recovery and long-term mucosal health. The Mayo Clinic provides detailed guidance on recognizing throat symptoms and determining when professional evaluation is necessary.
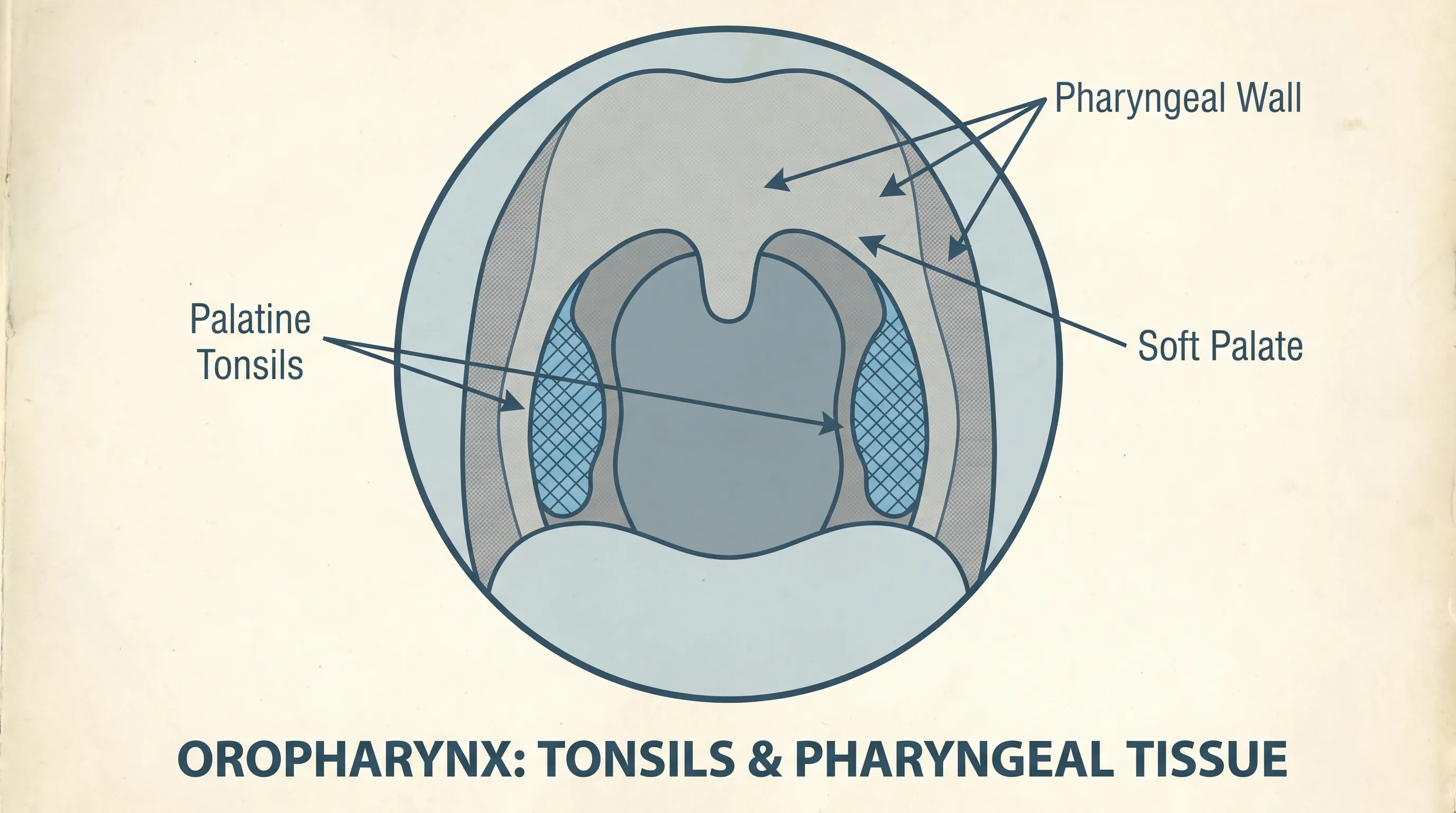
The oropharynx is a complex anatomical region where the respiratory and digestive tracts intersect, lined with delicate mucosal tissue that serves as a first line of defense against environmental pathogens, allergens, and irritants. When this protective barrier is compromised, inflammatory responses can manifest as localized exudate, cellular debris, or fungal proliferation that appears as pale or whitish areas. These visual changes rarely occur in isolation; they are typically accompanied by a constellation of systemic or localized symptoms that provide valuable diagnostic clues. By examining the physiological mechanisms, risk factors, and clinical presentations, you can make informed decisions about symptom management, treatment pathways, and preventive strategies tailored to your individual health profile.
Understanding the Anatomy and Physiology of Oropharyngeal Tissue
The posterior pharynx and palatine tonsils are integral components of Waldeyer's ring, a lymphatic tissue network strategically positioned to intercept inhaled or ingested microorganisms before they penetrate deeper into the respiratory and gastrointestinal systems. The tonsils are covered by stratified squamous epithelium and feature deep crypts that increase surface area for immune surveillance. These crypts naturally trap bacteria, dead cells, mucus, and food particles, which are normally cleared by ciliary action, salivary enzymes, and swallowing mechanics. When clearance mechanisms are disrupted, accumulated material undergoes calcification or bacterial overgrowth, leading to visible plaque formation.
Free calculatorWater Intake CalculatorCalculate daily water needsOpen the calculatorThe mucosal lining contains a rich vascular supply and numerous minor salivary glands that maintain tissue hydration and deliver antimicrobial proteins like lysozyme and lactoferrin. Disruptions in salivary flow, pH balance, or local immune function can alter the microbiome, creating an environment where opportunistic organisms thrive. This ecological shift is a primary driver behind many cases of white blotches in back of throat, ranging from transient inflammatory responses to chronic infectious processes. Understanding this anatomical context clarifies why certain systemic conditions, medications, and lifestyle habits disproportionately affect throat health and why targeted interventions must address both local symptoms and underlying physiological imbalances.
Common Medical Conditions Associated with White Patches
Identifying the precise etiology of pharyngeal lesions requires a systematic approach, as multiple distinct pathologies can present with similar visual features. Clinical differentiation relies on symptom duration, accompanying systemic signs, patient demographics, and response to empirical therapies. Below is a detailed breakdown of the most prevalent conditions linked to these visible changes.
Bacterial Infections and Acute Tonsillitis
Acute bacterial tonsillitis remains one of the most frequent causes of exudative pharyngitis. Pathogens such as Streptococcus pyogenes, Staphylococcus aureus, and Fusobacterium species invade the epithelial surface, triggering a robust inflammatory cascade characterized by vasodilation, neutrophil migration, and fibrin deposition. The resulting purulent exudate coalesces into discrete or confluent white patches that adhere firmly to the tonsillar pillars. Patients typically report severe odynophagia, fever, cervical lymphadenopathy, and malaise. Diagnostic confirmation relies on rapid antigen testing or throat culture, with antibiotic therapy initiated promptly to prevent complications like rheumatic fever or peritonsillar abscess formation. The CDC outlines the clinical presentation and diagnostic standards for bacterial throat infections.
Streptococcal Pharyngitis
Group A streptococcus (GAS) is responsible for the majority of bacterial pharyngitis cases worldwide. Unlike viral etiologies, GAS infections frequently produce petechiae on the soft palate alongside prominent white exudates covering enlarged tonsils. The Centor score and McIsaac modification are widely utilized clinical decision tools that integrate age, temperature, cervical adenopathy, absence of cough, and tonsillar exudate to estimate bacterial probability. Evidence-based guidelines recommend a 10-day course of penicillin or amoxicillin as first-line therapy to eradicate the pathogen, reduce transmission, and mitigate suppurative and nonsuppurative sequelae. Current clinical recommendations from public health authorities emphasize completing the full antibiotic course to prevent resistance.
Oral Thrush (Candidiasis)
Oral candidiasis occurs when Candida albicans or other fungal species proliferate beyond normal commensal levels, often following disruption of oral flora by broad-spectrum antibiotics, corticosteroids, uncontrolled diabetes, or immunosuppressive therapies. The hallmark presentation involves creamy, curd-like white plaques that can be gently wiped away, revealing an erythematous or bleeding mucosal base underneath. While thrush commonly affects the buccal mucosa and tongue dorsum, it frequently extends to the posterior pharynx, producing white blotches in back of throat accompanied by a burning sensation, altered taste, or cottony mouth. Diagnosis is primarily clinical, though potassium hydroxide preparation or fungal culture may be utilized in refractory cases. Mayo Clinic details how oral thrush develops and its relationship to immune and metabolic factors.
Viral Etiologies and Infectious Mononucleosis
Epstein-Barr virus (EBV), cytomegalovirus (CMV), adenoviruses, and herpes simplex virus can all induce significant pharyngeal inflammation. Infectious mononucleosis classically presents with exudative tonsillitis, profound fatigue, hepatosplenomegaly, and atypical lymphocytosis. The white patches in EBV-associated pharyngitis tend to be thicker and more persistent than typical viral exudates, often lasting 10 to 14 days. Supportive management focuses on hydration, analgesics, and activity restriction, while avoiding ampicillin-class antibiotics that trigger maculopapular rashes in EBV-positive patients. Viral etiologies generally resolve spontaneously as host cellular immunity neutralizes the pathogen. The CDC provides comprehensive information on infectious mononucleosis transmission and symptom management.
Tonsilloliths (Tonsil Stones)
Tonsil stones are calcified aggregations of trapped debris, keratin, mucus, and bacterial biofilm that form within deep crypts. Unlike infectious exudates, tonsilloliths are non-adherent, gritty, and often dislodged spontaneously during coughing or swallowing. They frequently produce chronic halitosis, throat irritation, foreign body sensation, and intermittent dysphagia. Mechanical removal is generally reserved for symptomatic cases, with irrigation devices, low-pressure water rinses, or professional crypt cleaning employed under controlled conditions. Recurrent stone formation may indicate cryptic architecture anomalies, and surgical intervention like tonsillectomy or laser cryptolysis can be considered for quality-of-life preservation.
Leukoplakia and Precancerous Changes
Leukoplakia manifests as thickened, non-removable white patches on oral or pharyngeal mucosa that cannot be attributed to infection or trauma. It is strongly associated with chronic tobacco use, heavy alcohol consumption, and human papillomavirus (HPV) infection. Histopathological evaluation is mandatory, as a subset of leukoplakias exhibits dysplastic changes that progress to squamous cell carcinoma over time. Early detection through regular oral examinations, tobacco cessation, and HPV vaccination significantly reduces malignant transformation risk. Unlike infectious lesions, leukoplakia requires longitudinal monitoring and potentially surgical or laser ablation based on biopsy grading. The National Cancer Institute (NIH) highlights the critical importance of early histological evaluation for leukoplakia.
Differential Diagnosis: Benign vs. Serious Presentations
Accurately distinguishing between self-limiting inflammatory processes and conditions requiring immediate intervention prevents both overtreatment and dangerous delays. Clinical evaluation hinges on temporal patterns, systemic involvement, lesion characteristics, and patient risk profiles.
| Condition | Primary Characteristics | Typical Duration | Contagious | Primary Intervention |
|---|---|---|---|---|
| Viral Pharyngitis | Diffuse redness, mild exudate, cough, rhinorrhea | 5-10 days | Yes (High) | Supportive care, analgesics |
| Streptococcal Throat | Thick white patches, fever, tender nodes, no cough | 1-2 weeks | Yes (High) | Penicillin-class antibiotics |
| Oral Candidiasis | Curd-like removable plaques, burning, dry mouth | 1-2 weeks | Low | Topical/systemic antifungals |
| Tonsil Stones | Hard calcified debris, halitosis, foreign body sensation | Chronic/Recurrent | No | Gargling, irrigation, possible surgery |
| Leukoplakia | Adherent thick patches, non-removable, often painless | Persistent/Indefinite | No | Biopsy, monitoring, lesion removal |
| Peritonsillar Abscess | Unilateral swelling, uvular deviation, trismus, severe pain | Progressive | Low (Secondary) | Needle aspiration/drainage, IV antibiotics |
This comparative framework highlights that white blotches in back of throat are not a singular diagnosis but a clinical sign requiring contextual interpretation. Lesion mobility, tissue adherence, associated pain patterns, and systemic markers collectively guide appropriate triage and therapeutic selection.
Diagnostic Process and Clinical Evaluation
When self-care measures fail to yield improvement or symptoms escalate, structured clinical assessment becomes necessary. Primary care physicians and otolaryngologists utilize a stepwise diagnostic algorithm beginning with comprehensive history taking and physical examination. Clinicians document lesion morphology, distribution, mucosal integrity, cervical lymph node status, and systemic vital signs. Flexible nasolaryngoscopy may be employed to visualize submucosal structures, assess vocal cord mobility, and rule out laryngeal involvement.
Laboratory investigations frequently include rapid streptococcal antigen tests, complete blood counts with differential analysis, and infectious disease panels when viral or atypical pathogens are suspected. In persistent or atypical presentations, fungal cultures, Epstein-Barr serology, or HIV screening may be indicated. When lesions demonstrate suspicious features such as induration, ulceration, or failure to resolve within two to three weeks, tissue biopsy provides definitive histopathological classification. Imaging modalities like computed tomography or magnetic resonance imaging are reserved for suspected deep space infections, abscess evaluation, or oncological staging.
Evidence-based diagnostic pathways emphasize minimizing unnecessary testing while maintaining high sensitivity for serious pathology. Mayo Clinic's clinical approach to throat evaluation consistently advocates for symptom-driven testing rather than empirical broad-spectrum interventions, which disrupt microbiome equilibrium and promote antimicrobial resistance.
Evidence-Based Treatment Approaches
Therapeutic strategies are meticulously aligned with confirmed etiology to maximize efficacy, minimize adverse effects, and prevent recurrence. Antibiotic stewardship principles dictate that antimicrobial therapy should only be administered when bacterial infection is confirmed or highly probable. First-line agents for GAS pharyngitis include penicillin V or amoxicillin, with clindamycin or macrolides reserved for penicillin-allergic patients. Adherence to full-course regimens prevents relapse and eradicates residual bacterial reservoirs that can trigger immune-mediated complications.
Antifungal medications for candidiasis range from topical nystatin suspensions and clotrimazole troches to systemic fluconazole for moderate-to-severe or refractory disease. Dosing duration typically spans 7 to 14 days, with clinical response monitored via symptom resolution and plaque clearance. Underlying predisposing factors such as xerostomia, poorly controlled glycemia, or inhaled corticosteroid use must be addressed concurrently to prevent mycological relapse.
Viral infections remain inherently self-limiting, with management centered on symptomatic relief, adequate hydration, and rest. Nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen effectively modulate prostaglandin-mediated pain pathways and reduce fever. Corticosteroids may be considered in severe exudative cases to decrease mucosal edema and accelerate symptom resolution, though routine use remains controversial and should be individualized based on severity and comorbidities.
Surgical interventions are indicated for structural anomalies, recurrent infections meeting clinical criteria, or complications like obstructive sleep apnea. Tonsillectomy demonstrates high long-term success rates for chronic tonsillitis and refractory tonsilloliths, while coblation cryptolysis offers a tissue-sparing alternative for cryptic debris management. All procedural decisions involve thorough risk-benefit analysis, patient counseling, and postoperative care planning to optimize recovery trajectories. The CDC’s antibiotic stewardship initiatives reinforce the importance of targeted prescribing to safeguard long-term public health.
Home Management and Self-Care Strategies
While clinical treatments address underlying pathology, structured self-care protocols significantly accelerate mucosal healing, reduce discomfort, and restore functional swallowing. Implementing evidence-based home interventions creates a supportive microenvironment that facilitates natural immune clearance and tissue regeneration. The Cleveland Clinic recommends integrating these supportive measures alongside prescribed medical treatments.
Therapeutic Gargling and Mucosal Soothing
Warm saline gargles remain the cornerstone of symptomatic relief, leveraging osmotic gradients to reduce tissue edema, dislodge superficial debris, and modulate local inflammatory mediators. Dissolving half a teaspoon of non-iodized salt in eight ounces of warm water and gargling for thirty seconds three to four times daily maintains optimal mucosal hydration without disrupting epithelial integrity. For enhanced antimicrobial activity, diluted hydrogen peroxide solutions or baking soda rinses can be alternated, provided concentrations remain within safe limits to prevent chemical irritation.
Throat lozenges containing benzocaine, phenol, or menthol provide temporary analgesia by desensitizing sensory nerve endings. Patients should select sugar-free formulations to minimize cariogenic risk and avoid prolonged use beyond seven days to prevent medication-overuse pharyngopathy. Hydrating sprays with glycerin or hyaluronic acid create a protective mucosal barrier that reduces friction during swallowing and supports epithelial repair.
Nutritional Modifications and Environmental Optimization
Dietary adjustments play a crucial role in minimizing mechanical irritation and supporting immune recovery. Soft, non-acidic, and room-temperature foods reduce thermal and chemical stress on inflamed mucosa. Incorporating broths, smoothies, cooked cereals, and mashed vegetables ensures adequate caloric and micronutrient intake without triggering odynophagia. Avoiding spicy, highly salted, citrus-based, or rough-textured foods prevents microtrauma and prolongs discomfort.
Environmental humidity significantly impacts mucosal hydration levels. Utilizing cool-mist humidifiers, particularly during sleep or in dry climates, prevents desiccation of pharyngeal tissues and enhances ciliary function. Maintaining indoor humidity between forty and fifty percent reduces airborne irritant concentration and minimizes nocturnal mouth breathing, which exacerbates throat dryness and secondary inflammation. Consistent hydration through room-temperature water, herbal infusions, and electrolyte-balanced beverages sustains systemic perfusion and facilitates toxin clearance through renal pathways.

Prevention and Long-Term Throat Health
Sustaining optimal pharyngeal integrity requires proactive lifestyle modifications and consistent hygiene practices that disrupt pathogenic colonization cycles. Handwashing remains the single most effective preventive measure against respiratory and oral pathogen transmission. Proper technique involving soap, warm water, and twenty seconds of mechanical friction significantly reduces viral and bacterial load before mucosal contact occurs.
Dental hygiene directly impacts oropharyngeal microbial equilibrium. Regular brushing, flossing, tongue scraping, and antiseptic mouthwash utilization prevent supragingival plaque accumulation that harbors pathogenic reservoirs capable of ascending into the tonsillar crypts. Biannual professional dental cleanings and routine oral cancer screenings provide early detection opportunities and personalized preventive guidance.
Smoking cessation is paramount, as tobacco smoke contains thousands of cytotoxic compounds that paralyze respiratory cilia, impair mucociliary clearance, and induce squamous metaplasia that predisposes to chronic inflammation and dysplastic transformation. Alcohol moderation reduces systemic immunosuppression and maintains mucosal barrier integrity. Vaccination adherence, including influenza, pneumococcal, and HPV immunizations, provides robust immunological protection against common pharyngeal pathogens and oncogenic viral strains. The World Health Organization (WHO) and CDC strongly advocate for timely HPV vaccination to reduce oropharyngeal cancer risk-and-cervical-cancer).
Sleep optimization, stress management, and balanced nutrition form the physiological foundation of immune resilience. Chronic psychological stress elevates cortisol levels, which suppresses lymphocyte proliferation and antibody production, creating windows of susceptibility to opportunistic infections. Incorporating mindfulness practices, regular aerobic exercise, and nutrient-dense diets rich in zinc, vitamin C, and omega-3 fatty acids enhances mucosal defense mechanisms and accelerates recovery timelines when exposures occur.
Frequently Asked Questions
How long does it take for white patches in the throat to go away?
The healing timeline depends entirely on the underlying cause. Viral infections typically resolve within 7 to 10 days with supportive care, while bacterial infections like strep throat improve within 48 hours of starting antibiotics. Fungal infections such as oral thrush may require 1 to 2 weeks of consistent antifungal treatment. Persistent lesions lasting beyond two weeks warrant prompt medical evaluation to rule out chronic conditions or precancerous changes.
Can dehydration cause white patches on the tonsils?
While dehydration itself does not directly produce infectious white patches, it creates a dry mucosal environment that reduces saliva production. Saliva contains antimicrobial enzymes and immunoglobulins that naturally cleanse the oral cavity. Chronic dry mouth can allow bacteria and fungi to colonize more easily, potentially triggering tonsillar debris accumulation or secondary infections that appear as white lesions.
Are white blotches in the throat contagious?
Contagiousness depends on the etiology. Viral pharyngitis, bacterial strep throat, and mononucleosis are highly contagious and spread through respiratory droplets and direct contact. Tonsil stones and leukoplakia are non-infectious and cannot be transmitted to others. Oral thrush may spread in immunocompromised individuals or through prolonged contact, though it is generally considered less contagious than bacterial or viral infections.
Should I try to scrape white patches off my tonsils?
Self-scraping or aggressively removing throat lesions is strongly discouraged. Mechanical trauma to the mucosa can introduce bacteria, cause microtears, trigger bleeding, and worsen inflammation. If the patches are tonsil stones, gentle gargling with warm salt water is safer. If they are infectious plaques, removing them does not treat the underlying pathogen and may spread infection deeper into surrounding tissues.
When should I seek emergency care for throat symptoms?
Immediate medical attention is necessary if you experience difficulty breathing, stridor, severe drooling, inability to swallow saliva, high fever exceeding 103°F (39.4°C), trismus (lockjaw), or a rapidly enlarging neck mass. These symptoms may indicate airway compromise, deep neck space infection, or peritonsillar abscess, which are medical emergencies requiring urgent evaluation and possible intervention.
Conclusion
Observing white blotches in back of throat can initially provoke concern, but a systematic understanding of potential causes transforms anxiety into informed action. The presence of these lesions spans a broad clinical spectrum, ranging from benign, self-limiting inflammatory responses to conditions requiring targeted medical intervention. By recognizing accompanying symptom patterns, respecting diagnostic boundaries, and adhering to evidence-based treatment protocols, you can effectively navigate recovery while preserving long-term oropharyngeal health.
Prioritizing mucosal hygiene, maintaining optimal hydration, implementing structured preventive habits, and seeking timely professional evaluation when symptoms deviate from expected recovery trajectories ensures comprehensive care. Remember that persistent, worsening, or functionally impairing lesions require thorough clinical assessment to exclude serious pathology. With appropriate guidance and consistent self-care, most pharyngeal conditions resolve completely, restoring comfort, swallowing function, and overall well-being. Trust the healing process, follow medical recommendations diligently, and maintain proactive health practices to safeguard your throat and respiratory system for years to come.
How we work
Researched and drafted with AI assistance, then reviewed by a human editor against the cited sources.
This article is general health information, not medical advice. Consult a qualified healthcare professional about your own situation.