Ear Crackling Sound: Causes, Diagnosis, and Expert Treatment Guide

Have you ever experienced a sudden, rhythmic popping or an ear crackling sound when swallowing, yawning, or simply turning your head? You are not alone. This common auditory sensation can range from a mild annoyance to a persistent symptom that disrupts concentration and sleep. While often dismissed as a trivial quirk of human anatomy, an ear crackling sound can signal a variety of underlying physiological processes, some completely harmless and others requiring professional intervention. Understanding why this phenomenon occurs is the first step toward relief and optimal ear health. In this comprehensive guide, we will explore the complex anatomy behind the symptom, identify the most frequent culprits, outline diagnostic pathways, and provide evidence-based treatment strategies. Whether you are a frequent air traveler dealing with altitude changes, someone managing seasonal allergies, or simply curious about your body’s mechanics, you will find actionable insights here. By the end of this article, you will know exactly when to monitor the situation, which home techniques are scientifically supported, and what clinical options can permanently resolve persistent discomfort. Let us dive into the mechanics of your auditory system and demystify why that familiar crackling sound occurs in the first place.
The Complex Anatomy and Mechanics Behind Auditory Crackling
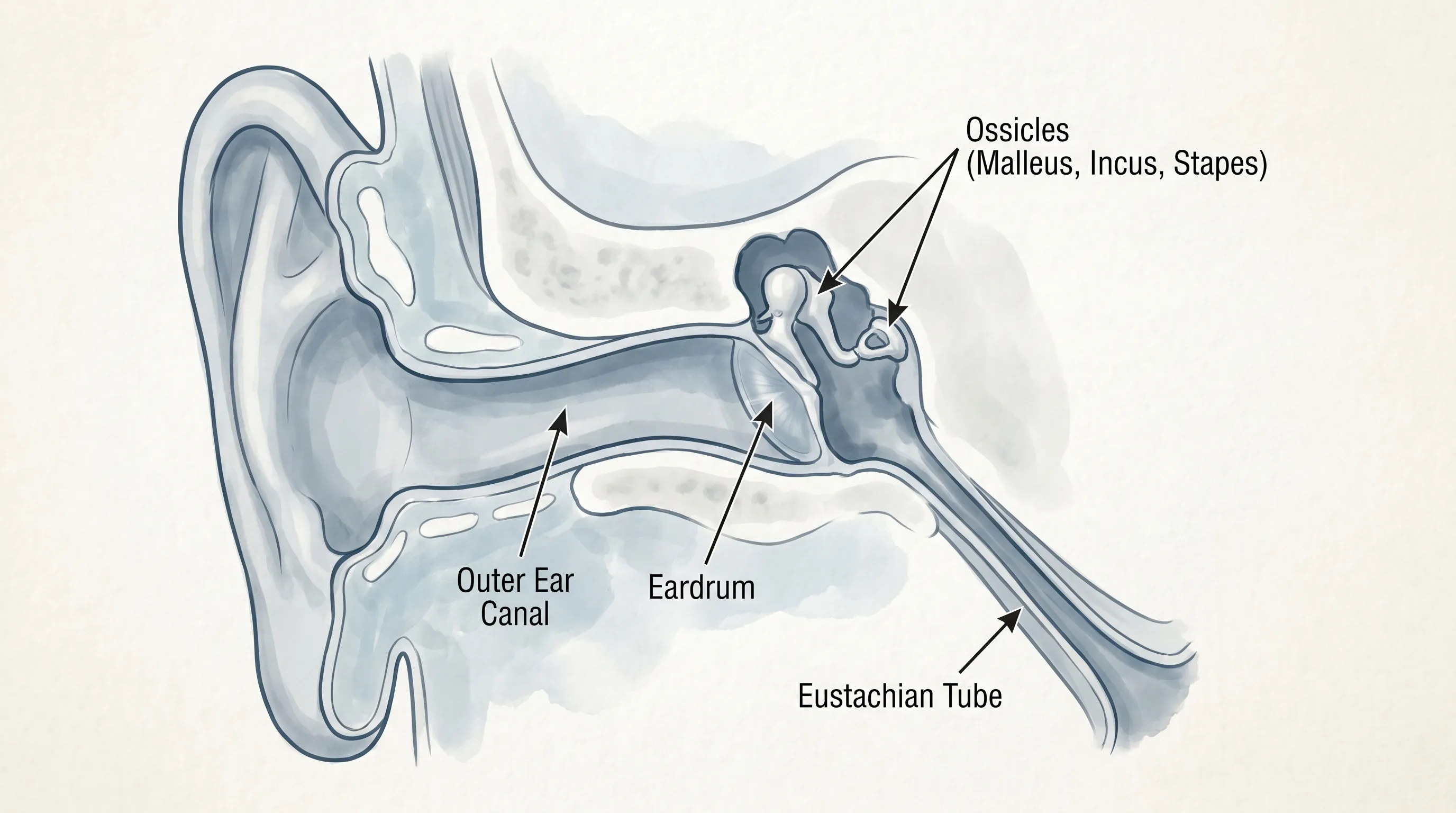
To effectively manage any auditory symptom, we must first understand the biological machinery responsible for generating it. The human ear is a marvel of evolutionary engineering, divided into three distinct sections: the outer, middle, and inner ear. Each plays a specialized role in sound conduction, balance, and pressure regulation, and dysfunction in any single component can manifest as an ear crackling sound.
Free calculatorWater Intake CalculatorCalculate daily water needsOpen the calculatorThe Eustachian Tube and Pressure Equalization
The most common source of crackling originates from the Eustachian tube, a narrow cartilage-lined channel connecting the middle ear to the nasopharynx. Under normal conditions, this tube remains closed to protect the middle ear from nasopharyngeal secretions and excessive noise. However, it briefly opens during swallowing, yawning, or chewing to ventilate the middle ear cavity and equalize atmospheric pressure across the tympanic membrane. When the mucosal lining becomes inflamed or swollen due to illness, allergies, or anatomical variations, the tube struggles to open smoothly. The resulting negative pressure creates a vacuum effect, causing the delicate tissues and eardrum to flex inward. The audible pop or crackle occurs when the tube finally overcomes resistance and snaps open. Understanding Eustachian Tube Function provides detailed insights into the mucociliary clearance mechanisms that govern this process.
Cerumen Dynamics and Auditory Canal Physics
Earwax, or cerumen, is a natural protective substance produced by sebaceous and modified apocrine glands in the outer third of the auditory canal. It is slightly acidic, hydrophobic, and packed with antimicrobial peptides that trap dust, dead skin cells, and foreign debris. Healthy cerumen migrates outward naturally through jaw movements like talking and chewing. When migration slows or wax hardens, it can create a partial seal near the tympanic membrane. As the jaw moves or the head changes position, the wax shifts slightly, scraping against the canal walls or pressing intermittently against the eardrum. This mechanical friction generates the characteristic crinkling, crackling, or rustling noises that patients frequently report.
Middle Ear Fluids and Ossicular Mechanics
Behind the eardrum lies a tiny air-filled chamber housing the three ossicles: the malleus, incus, and stapes. These bones transmit sound vibrations from the tympanic membrane to the oval window of the cochlea. When fluid accumulates in this space, either from inflammation, infection, or Eustachian dysfunction, it alters the acoustic impedance of the middle ear. As the ossicles move against this dampened environment, or as tiny air bubbles form and collapse within the fluid, subtle mechanical noises are generated. These sounds can travel directly into the cochlea or be conducted through bone, creating the perception of internal crackling that seems to originate deep within the skull.
Primary Medical and Environmental Causes
Identifying the root cause is essential for targeted treatment. An ear crackling sound rarely occurs in isolation; it is almost always accompanied by specific physiological triggers that healthcare professionals can trace back to identifiable pathways.
Eustachian Tube Dysfunction and Chronic Congestion
Eustachian tube dysfunction remains the leading cause of intermittent or persistent crackling. It can be acute, lasting only a few days during a common cold, or chronic, persisting for months. Risk factors include chronic rhinosinusitis, allergic rhinitis, gastroesophageal reflux disease (LPR), obesity, and congenital anatomical narrowing. When the tube fails to ventilate properly, negative pressure builds, pulling the eardrum inward. This retraction creates stiffness in the ossicular chain and generates popping sounds with every pressure shift. Studies indicate that nearly 1 in 10 adults will experience symptomatic ETD at some point in their lifetime.
Cerumen Impaction and Improper Cleaning Habits
While the auditory canal is self-cleaning, many individuals inadvertently disrupt this process. Cotton swabs, ear picks, and even hearing aids or earbuds can push cerumen deeper into the canal, creating a firm plug. This impaction alters the resonance of the ear canal and can cause crackling when the wax shifts during jaw movement. Impacted earwax can also trap moisture behind it, creating an ideal environment for bacterial or fungal overgrowth, which may further exacerbate the sensation.
Allergic Rhinitis and Upper Respiratory Inflammation
Seasonal or perennial allergies trigger a systemic histamine response that causes mucosal edema throughout the upper respiratory tract. The Eustachian tube opening sits in the nasopharynx, making it highly susceptible to this swelling. Chronic postnasal drip can also irritate the tube’s mucosal lining, leading to excessive mucus production. Patients with unmanaged allergies frequently report an ear crackling sound that fluctuates with environmental triggers like pollen counts, dust mites, or pet dander. Allergy Management Guidelines emphasize early intervention to prevent middle ear complications.
Temporomandibular Joint Disorders and Referred Sensations
The TMJ sits just anterior to the ear canal, separated only by a thin layer of tissue and the external auditory meatus. When the TMJ capsule becomes inflamed or the articular disc displaces, the joint produces audible clicks, pops, or crepitus during mandibular movement. Because of the close anatomical proximity, the auditory system interprets these joint sounds as originating from the ear itself. TMJ-related crackling is typically exacerbated by teeth clenching, chewing hard foods, or prolonged stress-induced bruxism.
Middle Ear Effusion and Barotrauma
Otitis media with effusion (OME) involves sterile fluid accumulation in the middle ear following a resolved infection or prolonged ETD. The fluid acts as a dampening agent, and as air bubbles slowly escape or re-enter through a partially obstructed Eustachian tube, patients hear continuous popping or bubbling. Similarly, rapid changes in ambient pressure during flights, scuba diving, or mountain driving can cause barotrauma. The sudden pressure differential forces the Eustachian tube to work overtime, resulting in intense, repetitive crackling as the body attempts to re-establish equilibrium.
| Cause Category | Typical Sound Pattern | Common Accompanying Symptoms | Recommended First Step |
|---|---|---|---|
| Eustachian Tube Dysfunction | Intermittent popping, worse with swallowing/yawning | Ear fullness, mild muffled hearing, sinus pressure | Nasal saline irrigation, intranasal corticosteroids |
| Cerumen Impaction | Rustling, crinkling, constant faint crackle | Reduced hearing, ear fullness, occasional itch | Cerumenolytic drops, avoid cotton swabs |
| Allergic Rhinitis | Fluctuating crackling with environmental exposure | Sneezing, itchy/watery eyes, nasal congestion | Antihistamines, allergen avoidance, HEPA filtration |
| TMJ Dysfunction | Clicking/popping synchronized with jaw movement | Jaw pain, headaches, tooth wear, facial tension | Soft diet, warm compresses, dental evaluation |
| Barometric Pressure Shifts | Sudden intense crackling during altitude change | Acute pressure pain, temporary muffled hearing | Valsalva maneuver, pre-flight decongestants |
When to Seek Professional Medical Attention
While most episodes of an ear crackling sound resolve spontaneously, certain clinical presentations warrant prompt medical evaluation. Ignoring persistent symptoms can lead to chronic middle ear pathology, permanent hearing impairment, or tympanic membrane damage.
Red Flags Requiring Immediate Evaluation
Schedule an appointment with an otolaryngologist or primary care physician if you experience severe otalgia, sudden unilateral or bilateral hearing loss, vertigo, or spontaneous otorrhea. Purulent discharge suggests acute otitis media or tympanic membrane perforation. Persistent crackling lasting longer than three weeks despite conservative home measures may indicate structural ETD, chronic serous effusion, or rare conditions like patulous Eustachian tube. Additionally, crackling accompanied by pulsatile tinnitus (synchronized with the heartbeat) should be investigated promptly to rule out vascular abnormalities or glomus tumors.
Long-Term Risks of Untreated Middle Ear Dysfunction
Chronic negative pressure in the middle ear can cause tympanic membrane retraction pockets. Over time, these weakened areas may accumulate keratin debris, leading to cholesteatoma formation, which requires surgical intervention. Repeated fluid accumulation increases the risk of adhesive otitis media, where scar tissue fuses the eardrum to the ossicles, permanently impairing conductive hearing. Early diagnosis prevents irreversible structural damage and preserves auditory function.
Differentiating Mechanical Crackling from Neurological or Vascular Sounds
It is crucial to distinguish benign mechanical crackling from pathological tinnitus or vascular bruits. Mechanical sounds typically change with swallowing, yawning, or head movement. In contrast, sensorineural tinnitus is often high-pitched, constant, and unaffected by jaw or neck motion. Vascular pulsations follow the cardiac cycle and may indicate carotid artery stenosis or arteriovenous malformations. A thorough clinical history and physical examination can reliably differentiate these etiologies.
Diagnostic Pathways and Clinical Evaluation
Modern otolaryngology employs a multi-modal diagnostic approach to pinpoint the exact mechanism behind auditory symptoms. Clinical evaluation typically progresses from non-invasive examination to specialized functional testing.
Pneumatic Otoscopy and Endoscopic Visualization
The cornerstone of diagnosis is pneumatic otoscopy. Using a specialized otoscope that delivers gentle puffs of air, clinicians observe the tympanic membrane’s mobility. A retracted, stiff, or fluid-dampened eardrum fails to respond normally, indicating ETD or effusion. Nasal endoscopy allows direct visualization of the Eustachian tube orifice, revealing polyps, severe edema, or secretory blockage. This minimally invasive procedure takes minutes and provides immediate diagnostic clarity.
Tympanometry and Pure Tone Audiometry
Tympanometry measures middle ear compliance by varying ear canal pressure and recording tympanic membrane movement. A Type B flat curve suggests fluid accumulation or perforation, while a Type C negative-pressure peak indicates Eustachian tube blockage. Pure tone audiometry quantifies hearing thresholds across frequencies, identifying conductive vs. sensorineural deficits. Audiometric Testing Standards outline standardized protocols used globally for accurate auditory assessment.
Advanced Imaging and Refractory Cases
When symptoms persist despite conservative therapy, high-resolution CT scans of the temporal bones evaluate ossicular chain integrity, mastoid air cell aeration, and bony Eustachian tube anatomy. MRI may be ordered if neurological or vascular etiologies are suspected. In complex TMJ cases, panoramic radiography or cone-beam CT helps assess joint morphology. Multidisciplinary collaboration between ENT specialists, audiologists, and dental professionals ensures comprehensive care.
Evidence-Based Treatment Options and Medical Interventions
Treatment strategies depend entirely on the underlying etiology. Clinicians prioritize conservative measures before progressing to procedural or surgical interventions.
Pharmacological Management Strategies
For inflammatory causes like allergies or post-viral swelling, intranasal corticosteroids (e.g., fluticasone, budesonide) reduce mucosal edema and improve tube patency. Oral decongestants containing pseudoephedrine may provide short-term relief for acute barotrauma or sinus congestion but are contraindicated in hypertension and should not exceed three days. Antibiotics are reserved only for confirmed bacterial otitis media, as they offer no benefit for sterile effusion or mechanical ETD. Mucolytics and antihistamines may help clear thick secretions but should be used under medical supervision.
Professional Earwax Removal Techniques
Impacted cerumen requires careful extraction to avoid canal trauma or tympanic perforation. Otologists typically use microscopic visualization combined with microsuction, which gently aspirates wax without introducing water. Alternatively, controlled irrigation with body-temperature saline effectively flushes out softened plugs. Cerumenolytic agents containing carbamide peroxide, glycerin, or mineral oil are prescribed for three to five days prior to irrigation. Self-administered irrigation should never be attempted in patients with a history of eardrum perforation, ear surgery, or active infection.
Surgical and Minimally Invasive Procedures
Chronic ETD refractory to medication may benefit from Eustachian tube balloon dilation. This FDA-approved procedure involves inserting a catheter into the tube, inflating it to remodel the cartilaginous portion, and restoring natural ventilation. For recurrent middle ear effusion, pressure-equalizing (PE) tubes bypass the obstructed Eustachian tube, allowing continuous pressure equalization and fluid drainage. TMJ-related crackling often improves with custom occlusal splints, physical therapy focusing on myofascial release, and behavioral modifications to reduce bruxism.
Practical Home Remedies and Self-Care Strategies
Most cases of an ear crackling sound respond well to conservative, evidence-based self-management techniques. Implementing these strategies consistently can accelerate recovery and prevent recurrence.
The Valsalva and Toynbee Maneuvers for Pressure Equalization
The Valsalva maneuver involves closing the mouth, pinching the nostrils shut, and gently exhaling against the closed airway. This increases nasopharyngeal pressure, forcing the Eustachian tubes open. It should be performed gently to avoid barotrauma; forceful blowing can rupture the eardrum. The Toynbee maneuver (pinching the nose and swallowing simultaneously) creates negative pressure in the nasopharynx, which can also open the tubes. Both techniques are highly effective during air travel, elevator rides, or mountain driving. Practice them before discomfort arises to establish muscle memory.
Hydration, Nutrition, and Environmental Modifications
Systemic hydration thins respiratory mucus, making it easier for the Eustachian tube to clear secretions. Aim for at least eight to ten glasses of water daily. Omega-3 fatty acids and vitamin C possess anti-inflammatory properties that support mucosal health. Use a clean, cool-mist humidifier in dry environments to prevent nasal mucosa from drying and crusting, which exacerbates tube blockage. Reduce exposure to tobacco smoke, strong chemical fumes, and excessive caffeine, as these can impair ciliary function and increase mucosal edema.

Safe Cleaning Practices and What to Avoid
Never insert cotton swabs, bobby pins, or keys into the auditory canal. These objects remove protective cerumen from the outer third while compacting the remainder against the eardrum, worsening impaction. Avoid commercial ear candles entirely; they lack clinical efficacy and pose severe burn and canal occlusion risks. If you use hearing aids, earbuds, or protective earplugs, clean them daily and allow the ears to rest for several hours daily to restore natural ventilation. Regularly change filters in air purifiers and vacuum carpets to minimize allergen exposure that triggers Eustachian inflammation.
Frequently Asked Questions
What causes that crackling noise in my ear when I swallow?
When you swallow, the muscles attached to the Eustachian tube contract, briefly opening it to equalize pressure. If the tube is swollen, congested, or surrounded by thick mucus, the opening process becomes uneven. The tissue snaps or the mucus bubbles, producing the crackling sound. This is usually harmless and resolves as inflammation decreases.
Can stress or anxiety make an ear crackling sound worse?
Yes. Psychological stress elevates cortisol and adrenaline levels, which can trigger jaw clenching, teeth grinding, and increased muscle tension around the temporomandibular joint and neck. This tension alters Eustachian tube dynamics and amplifies auditory awareness, making you hyper-focused on normal physiological sounds. Stress management techniques like diaphragmatic breathing and progressive muscle relaxation can significantly reduce symptom perception.
How long does it take for Eustachian tube crackling to resolve?
Acute viral-related ETD typically resolves within 7 to 14 days as mucosal swelling subsides. Allergy-driven or chronic structural ETD may persist for weeks or months and often requires ongoing management with nasal sprays or procedural intervention. If symptoms exceed three weeks without improvement, consult an ENT specialist to rule out persistent effusion or anatomical obstruction.
Is it safe to use ear drops when experiencing crackling sounds?
Over-the-counter cerumenolytic drops are safe if wax impaction is confirmed or suspected. However, avoid any drops containing alcohol, hydrogen peroxide, or antibiotic additives unless prescribed by a physician, especially if you have a perforated tympanic membrane or ear tubes. Always warm drops to body temperature before administration to prevent vertigo.
Can flying or scuba diving permanently damage my ears from constant crackling?
Frequent pressure changes without proper equalization can cause cumulative barotrauma, leading to tympanic membrane scarring, chronic effusion, or sensorineural hearing loss. Always pre-medicate with a decongestant if congested before flying or diving, and use the Valsalva maneuver frequently during descent. Never dive with active sinus congestion or severe ETD, as the risk of permanent middle ear injury is significantly elevated.
Conclusion
Experiencing an ear crackling sound can be unsettling, but it is rarely a sign of serious pathology when it occurs in isolation. By understanding the intricate relationship between your Eustachian tubes, cerumen dynamics, and surrounding musculoskeletal structures, you can identify triggers and implement targeted interventions. Most cases resolve with conservative home care, proper hygiene, and environmental modifications. However, persistent symptoms accompanied by pain, hearing changes, or dizziness warrant prompt professional evaluation to prevent long-term complications. Armed with accurate diagnostic knowledge and evidence-based treatment strategies, you can confidently navigate auditory discomfort and protect your hearing health. Prioritize early intervention, avoid harmful self-cleaning practices, and consult qualified otolaryngology professionals when symptoms persist. Your ears play a vital role in communication, balance, and overall well-being, and attentive care ensures they continue functioning optimally for years to come.
How we work
Researched and drafted with AI assistance, then reviewed by a human editor against the cited sources.
This article is general health information, not medical advice. Consult a qualified healthcare professional about your own situation.