Can Dry Eyes Cause Headaches? Medical Insights, Symptoms & Relief Strategies
If you have ever experienced a persistent, dull ache behind your eyes after hours of reading, working on a computer, or driving, you might be wondering whether the source of your discomfort is actually visual. Many patients present to clinics asking whether dry eyes can cause headaches, and the short medical response is a definitive yes. While headaches are commonly attributed to stress, dehydration, or neurological conditions, ocular surface disease represents an underrecognized but highly prevalent trigger. The intricate network of nerves connecting the cornea, lacrimal glands, and cranial structures means that even mild tear film instability can cascade into significant craniofacial pain. Understanding the physiological mechanisms behind this phenomenon, identifying the precise symptoms, and implementing evidence-based management strategies can dramatically improve quality of life. This comprehensive guide explores the clinical relationship between dry eye syndrome and cephalgia, providing actionable insights, diagnostic criteria, and long-term prevention protocols backed by peer-reviewed research and ophthalmological guidelines.
The Physiological Connection Between Ocular Surface Disease and Cephalgia
The human eye is one of the most densely innervated structures in the body. The cornea contains over seven thousand sensory nerve endings per square millimeter, making it exquisitely sensitive to changes in temperature, moisture, and chemical composition. When the tear film destabilizes or evaporates too quickly, these nociceptors fire excessively, sending distress signals through the ophthalmic branch of the trigeminal nerve. This pathway does not terminate locally; instead, it converges in the trigeminal ganglion and brainstem, where pain processing centers interpret the input. Over time, sustained peripheral sensitization leads to central sensitization, meaning the brain begins to generate pain signals even after the initial ocular trigger has been removed. This neurobiological cascade explains why patients frequently question whether dry eyes can cause headaches, as the referred pain often manifests in the frontal, temporal, or retro-orbital regions.
Free calculatorHeadache Location ChartIdentify headache types by locationOpen the calculatorHow Tear Film Instability Triggers Referred Pain
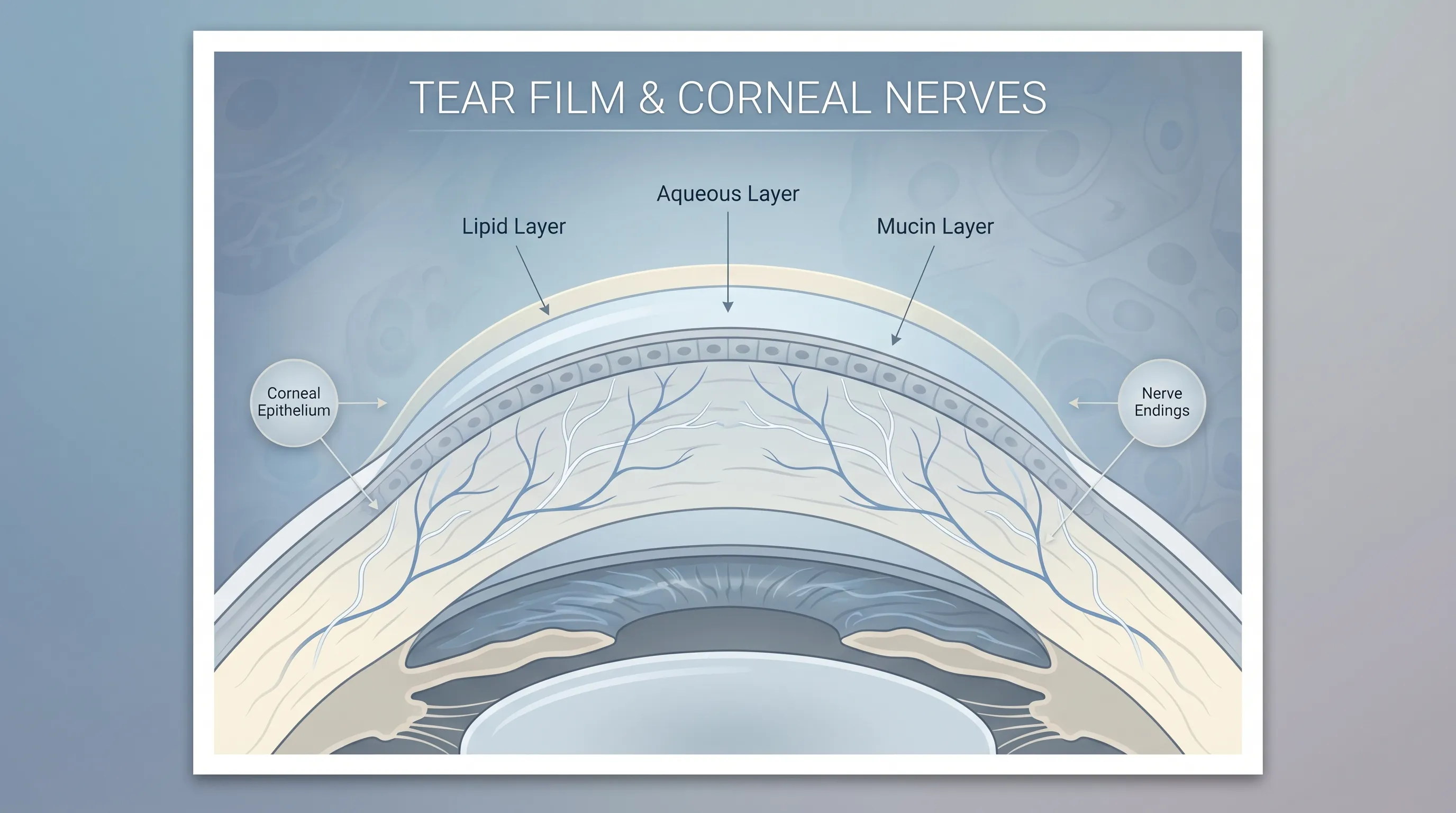
A healthy tear film consists of three distinct layers: a mucin layer that adheres tears to the ocular surface, an aqueous layer that provides hydration and oxygen, and a lipid layer that prevents evaporation. Dysfunction in any single component disrupts the entire system. For example, meibomian gland dysfunction reduces lipid production, causing rapid tear evaporation. As the ocular surface desiccates, epithelial micro-erosions develop, exposing nerve endings directly to air and inflammatory mediators. The resulting inflammatory response releases cytokines such as interleukin-6 and tumor necrosis factor-alpha, which further lower the threshold for pain transmission. Studies published by the American Academy of Ophthalmology demonstrate that patients with moderate to severe dry eye disease report headache frequencies three times higher than those with stable tear films. When evaluating whether dry eyes can cause headaches, clinicians often find that improving tear film osmolarity directly reduces headache severity within weeks of targeted therapy.
The Role of the Trigeminal Nerve and Ocular Reflex Arcs
Beyond direct pain referral, dry eyes activate protective reflex arcs that contribute to muscular tension. The trigeminofacial reflex triggers involuntary squinting, brow contraction, and sustained contraction of the orbicularis oculi and frontalis muscles. While initially designed to protect the cornea from exposure and foreign bodies, chronic activation transforms these muscle contractions into persistent tension. Overworked periorbital and extraocular muscles generate lactic acid buildup and trigger point development, mimicking the clinical presentation of tension-type headaches. Research from the National Eye Institute (NIH) highlights that patients with chronic dry eye often exhibit measurable increases in pericranial muscle tenderness and reduced cervical flexibility. This neuromuscular fatigue explains why individuals who spend extended periods focusing on detailed tasks without adequate lubrication frequently develop a heavy, band-like sensation across the forehead and upper neck.
Common Triggers and Underlying Risk Factors
Identifying the specific catalysts behind ocular dryness and subsequent cranial pain is essential for targeted management. Environmental exposures, behavioral habits, pharmacological agents, and systemic health conditions all interact to compromise tear film integrity. By mapping these variables, patients can proactively modify their surroundings and routines to interrupt the headache cycle before it fully develops.
Digital Eye Strain and the Modern Screen Lifestyle
Prolonged visual attention to digital displays fundamentally alters blinking patterns. Under normal conditions, humans blink approximately fifteen to twenty times per minute, distributing tears evenly across the cornea. During intense screen focus, blink rate can drop by up to sixty percent, and incomplete blinking becomes prevalent. This behavioral adaptation leaves the inferior corneal surface exposed, accelerating evaporation and triggering localized inflammation. The constant demand for accommodative focus from the ciliary muscles compounds the issue, leading to asthenopia, which frequently presents as frontal headache. Comprehensive reviews from the Mayo Clinic confirm that digital eye strain is now the leading contributor to secondary dry eye complaints in adults under fifty. Implementing structured visual breaks, optimizing screen positioning, and utilizing blue-light filtering or anti-reflective coatings can significantly reduce blink suppression and muscular fatigue.
Environmental Exposures and Climate Factors
Ambient conditions play a surprisingly dominant role in ocular surface hydration. Low relative humidity, high wind velocity, air conditioning systems, and indoor heating strips moisture from the tear film. Aircraft cabins, for instance, often maintain humidity levels below fifteen percent, which is profoundly desiccating. Similarly, urban environments with high particulate matter and allergens stimulate reflex tearing that paradoxically washes away essential lipid and mucin layers, leaving a deficient aqueous base. Seasonal allergies exacerbate inflammation through histamine release, causing vasodilation, redness, and heightened nerve sensitivity. According to CDC environmental health resources, patients living in arid climates or working in poorly ventilated offices frequently report a consistent correlation between environmental exposure and headache onset. Utilizing desktop humidifiers, avoiding direct airflow from vents, and wearing wraparound protective eyewear outdoors can create a localized microenvironment that preserves tear stability.
Systemic Health Conditions and Pharmacological Contributors
Dry eye syndrome rarely exists in isolation; it is frequently a manifestation of broader physiological changes. Autoimmune disorders such as Sjögren’s syndrome, rheumatoid arthritis, and lupus directly attack exocrine glands, severely reducing lacrimal and salivary secretions. Hormonal fluctuations, particularly during menopause, decrease androgen levels that are crucial for meibomian gland function. Additionally, numerous prescription and over-the-counter medications carry anticholinergic properties that reduce tear production. Common culprits include antihistamines, decongestants, antidepressants, beta-blockers, and acne medications containing retinoids. Understanding your medication profile is a critical step when exploring whether dry eyes can cause headaches, as adjusting dosages under medical supervision often resolves both the ocular and cranial symptoms simultaneously. Guidelines from the Cleveland Clinic emphasize reviewing medication lists as a primary intervention for refractory ocular surface disease.
Clinical Differentiation: Identifying Dry Eye Related Headaches
Accurately distinguishing dry eye-induced headaches from primary headache disorders or other secondary causes requires careful symptom analysis. The presentation often overlaps with tension-type headaches, but specific accompanying ocular signs provide diagnostic clarity. Recognizing these patterns prevents misdiagnosis and ensures appropriate intervention.
Distinguishing Tension-Type from Migraine Phenotypes
Tension-type headaches originating from ocular strain typically manifest as bilateral, non-pulsating pressure that intensifies throughout the day. They lack the nausea, vomiting, photophobia, and phonophobia characteristic of migraines, though severe dry eye cases can occasionally trigger light sensitivity due to corneal nerve hypersensitivity. Migraines are often preceded by neurological auras and involve neurovascular inflammation, whereas dry eye headaches correlate directly with visual tasks, environmental dryness, and time spent focusing without blinking. Keeping a symptom diary that tracks headache onset, screen duration, environmental conditions, and response to lubricating drops can reveal unmistakable patterns. Clinical guidelines recommend this behavioral tracking as a first-line diagnostic tool before initiating pharmacological treatment.
Associated Ocular Symptoms and Neurological Overlap
Dry eye headaches are rarely isolated; they are accompanied by a constellation of ocular complaints that reinforce the diagnosis. Patients consistently report a gritty, sandy, or burning sensation, intermittent blurry vision that clears upon blinking, excessive tearing as a reflex response to irritation, and difficulty wearing contact lenses for extended periods. Some individuals also experience a sensation of heaviness around the eyelids or mild photophobia. The neurological overlap occurs because the trigeminal nerve innervates both the meninges and the ocular surface, meaning central sensitization can blur the lines between ocular and cranial pain. When addressing the question of whether dry eyes can cause headaches, clinicians look for this symptom cluster. If lubrication provides partial or complete headache relief, the diagnosis is strongly supported.
| Symptom Category | Dry Eye-Related Headache | Primary Migraine | Tension-Type Headache | Sinusitis Headache |
|---|---|---|---|---|
| Pain Quality | Dull, aching, band-like pressure | Throbbing, pulsating, often unilateral | Steady, squeezing, bilateral | Dull pressure, often facial/cheek |
| Ocular Indicators | Grittiness, burning, reflex tearing, fluctuating vision | Aura, photophobia, phonophobia | Mild periorbital tenderness | Nasal congestion, purulent discharge |
| Aggravating Factors | Screen time, wind, dry air, prolonged reading | Stress, hormonal shifts, certain foods | Poor posture, neck strain, fatigue | Weather changes, allergies, colds |
| Relief Triggers | Artificial tears, blinking, rest, humidifier | Triptans, dark quiet room, hydration | OTC analgesics, massage, relaxation | Decongestants, nasal irrigation, rest |
Professional Diagnosis and Diagnostic Pathways
While self-management strategies provide initial relief, a formal evaluation ensures underlying conditions are not overlooked. Ophthalmologists and optometrists utilize standardized testing to quantify tear production, assess evaporation rates, and visualize meibomian gland structure. These diagnostics form the foundation of personalized treatment plans.
Comprehensive Tear Film and Ocular Surface Evaluation
The diagnostic workflow typically begins with a detailed patient history and symptom questionnaire, such as the OSDI (Ocular Surface Disease Index). Clinicians then perform the Schirmer test to measure basal tear secretion and the tear breakup time (TBUT) test to evaluate lipid layer stability. Non-invasive keratograph devices and infrared meibography provide high-resolution images of gland dropout, while vital dyes like fluorescein and lissamine green highlight epithelial damage under cobalt blue light. Corneal sensitivity testing and osmolarity measurements further refine the diagnosis. According to the Tear Film & Ocular Surface Society and NIH clinical standards, combining these modalities yields over ninety percent diagnostic accuracy. If you are investigating whether dry eyes can cause headaches, a comprehensive exam rules out glaucoma, optic neuritis, and intracranial pathologies that mimic similar symptoms.
When to Seek Specialized Neurological or Ophthalmological Care
Persistent headaches accompanied by sudden vision loss, severe ocular pain, double vision, or pupillary abnormalities require immediate specialist evaluation. Red flag symptoms suggest conditions such as acute angle-closure glaucoma, temporal arteritis, or increased intracranial pressure, which demand urgent intervention. Additionally, if symptoms do not improve after four to six weeks of consistent over-the-counter management and lifestyle modification, referral to a dry eye specialist or neuro-ophthalmologist is warranted. Advanced cases may benefit from multidisciplinary care that integrates optometry, neurology, and rheumatology, particularly when autoimmune markers are elevated. Early specialist involvement prevents chronic pain syndromes and irreversible ocular surface damage.
Evidence-Based Treatment Modalities and Relief Protocols
Effective management requires a tiered approach that addresses inflammation, tear deficiency, evaporative loss, and neuromuscular tension. Clinical guidelines recommend starting with conservative measures before advancing to prescription therapies and procedural interventions.
First-Line Therapies and Over-the-Counter Solutions
Preservative-free artificial tears remain the cornerstone of daily management. Unlike preserved formulations, which can exacerbate epithelial toxicity with frequent use, preservative-free vials provide pure lubrication that stabilizes the tear film without cellular damage. Glycerin-based and carboxymethylcellulose drops offer short-term comfort, while lipid-replenishing emulsions target evaporative dry eye specifically. Warm compresses applied for ten minutes twice daily liquefy meibomian secretions, restoring the critical oily layer. Gentle lid massage following application expresses trapped debris and improves gland outflow. Patients consistently report significant headache reduction within ten to fourteen days of disciplined adherence to this regimen.
Prescription Medications and Advanced Clinical Procedures
When conservative measures prove insufficient, clinicians escalate to targeted pharmacotherapy. Topical cyclosporine (Restasis) and lifitegrast (Xiidra) modulate T-cell mediated inflammation, addressing the root cause of chronic dry eye rather than merely masking symptoms. Corticosteroid drops provide rapid short-term anti-inflammatory action but require careful monitoring due to intraocular pressure risks. Autologous serum tears, derived from the patient’s own blood, deliver growth factors and vitamins that accelerate epithelial healing in severe cases. Procedural interventions include punctal plugs, which physically block tear drainage, and intense pulsed light (IPL) therapy, which reduces gland inflammation and bacterial load. For refractory headaches stemming from ocular strain, some neurologists prescribe muscle relaxants or neuromodulators alongside ocular surface treatment, acknowledging the bidirectional relationship between eye health and cranial pain. Exploring whether dry eyes can cause headaches ultimately leads to personalized protocols that restore tear film equilibrium and break the neuroinflammatory cycle.
Sustainable Prevention Strategies and Long-Term Eye Health
Preventing recurrence requires embedding ocular hygiene into daily routines. Long-term eye health depends on environmental control, behavioral modification, nutritional support, and regular professional monitoring. These sustainable habits protect the tear film and reduce the frequency of dry eye-related cranial discomfort.
Ergonomic Optimization and Visual Hygiene Practices
Workspace configuration directly impacts blink rate and accommodative demand. Position the top of your monitor at or slightly below eye level to encourage a downward gaze, which naturally reduces the exposed ocular surface area and slows evaporation. Maintain a viewing distance of twenty to thirty inches, and adjust screen brightness to match ambient lighting, eliminating glare. Implement the 20-20-20 rule: every twenty minutes, look at an object twenty feet away for twenty seconds. This resets accommodative focus, encourages complete blinking, and relaxes periorbital muscles. Regular computer use combined with structured visual breaks significantly lowers the incidence of both ocular dryness and tension headaches.
Nutritional Support and Lifestyle Modifications
Systemic hydration and targeted nutrition profoundly influence tear quality. Consuming adequate daily water intake ensures proper lacrimal gland perfusion. Omega-3 fatty acids, particularly eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) from fish oil or flaxseed, inhibit inflammatory prostaglandins and improve meibum consistency. Clinical trials supported by the NIH Office of Dietary Supplements demonstrate that daily supplementation of two to three grams of high-quality omega-3 reduces dry eye severity and associated headache frequency. Limiting alcohol and caffeine intake prevents diuresis-induced dehydration, while incorporating vitamin A, D, and zinc supports epithelial integrity. Combined with adequate sleep and stress management through mindfulness or gentle exercise, these nutritional strategies create a physiological environment where tear film stability thrives.


Frequently Asked Questions
What is the exact mechanism linking dry eyes to headaches?
The connection primarily involves the trigeminal nerve, which supplies sensory fibers to both the ocular surface and the forehead. When tear film instability causes corneal dryness and nerve irritation, the brain interprets this as localized pain, which can radiate as tension-type or referred headaches. Chronic ocular surface inflammation further sensitizes these neural pathways, making headache development highly probable in severe cases.
How can I differentiate a dry eye headache from a migraine?
Migraines typically present with throbbing, unilateral pain, nausea, and sensitivity to light or sound, often accompanied by visual auras. Dry eye-related headaches are usually bilateral, described as a dull ache or tight band across the forehead or temples, and consistently worsen after prolonged screen use, reading, or exposure to dry environments. They are frequently accompanied by gritty, burning, or watery eye sensations that improve with lubrication.
Can over-the-counter artificial tears resolve dry eye-induced headaches?
Yes, preservative-free artificial tears can provide significant short-term relief by stabilizing the tear film and reducing corneal nerve irritation. However, if headaches persist beyond a few days of consistent use, or if you experience vision changes, severe pain, or photophobia, it indicates an underlying condition that requires prescription therapy or specialized clinical intervention.
Do contact lenses worsen the risk of developing headaches from dry eyes?
Contact lenses can exacerbate dry eye symptoms by disrupting natural tear exchange, absorbing moisture, and creating micro-abrasions on the cornea. This heightened ocular surface stress increases nerve sensitivity and muscle tension, significantly raising the likelihood of headaches. Switching to daily disposables, using rewetting drops approved for lens wear, or limiting wear time can mitigate this risk.
When should I consult a doctor for persistent eye pain and headaches?
Seek professional evaluation if symptoms interfere with daily activities, persist beyond one to two weeks despite consistent self-care, or are accompanied by blurred vision, severe light sensitivity, red eye, or sudden pain intensity. A comprehensive examination can rule out secondary conditions such as glaucoma, uveitis, or neurological disorders and establish a targeted treatment protocol.
Conclusion
The relationship between ocular surface disease and cranial pain is both anatomically logical and clinically well-documented. Patients frequently discover that addressing whether dry eyes can cause headaches leads them to a straightforward truth: stabilizing the tear film, reducing ocular inflammation, and modifying visual habits directly alleviate referred cranial discomfort. By combining evidence-based lubrication therapies, ergonomic optimization, nutritional support, and timely professional evaluation, individuals can effectively break the cycle of strain-induced headaches. Prioritizing proactive eye care not only enhances visual comfort but also serves as a powerful preventive strategy against chronic pain syndromes. For those experiencing persistent symptoms, consulting an ophthalmologist or optometrist ensures accurate diagnosis and personalized management. Ultimately, sustainable relief lies in understanding the interconnected nature of ocular health and neurological function, empowering patients to implement lasting, physician-guided solutions for a clearer, pain-free daily experience. For additional clinical resources and patient education materials, refer to the American Academy of Ophthalmology guidelines, explore the National Eye Institute's comprehensive dry eye research, and review peer-reviewed treatment protocols via the Mayo Clinic's patient portal.
How we work
Researched and drafted with AI assistance, then reviewed by a human editor against the cited sources.
This article is general health information, not medical advice. Consult a qualified healthcare professional about your own situation.